
EMERGENCY ROOM DEATH BINGO
How to impolitely refuse to be sent home to die


The ER has a unique mission: to keep you from dying right now.
Bleeding out? Flopping on the floor like a psychotic fish? You’re in the right place.
But if your symptoms or injuries aren’t dramatically life-threatening, they may default to cutting you loose—sending you home.
Possibly sending you home to die.
Cryptically ill: Serious conditions, vague symptoms
Bring a medical puzzle to the emergency room and you’re in trouble.
It’s the department of fierce ‘n’ fast medical heroics—not long-haul deep dives into medical complexity.
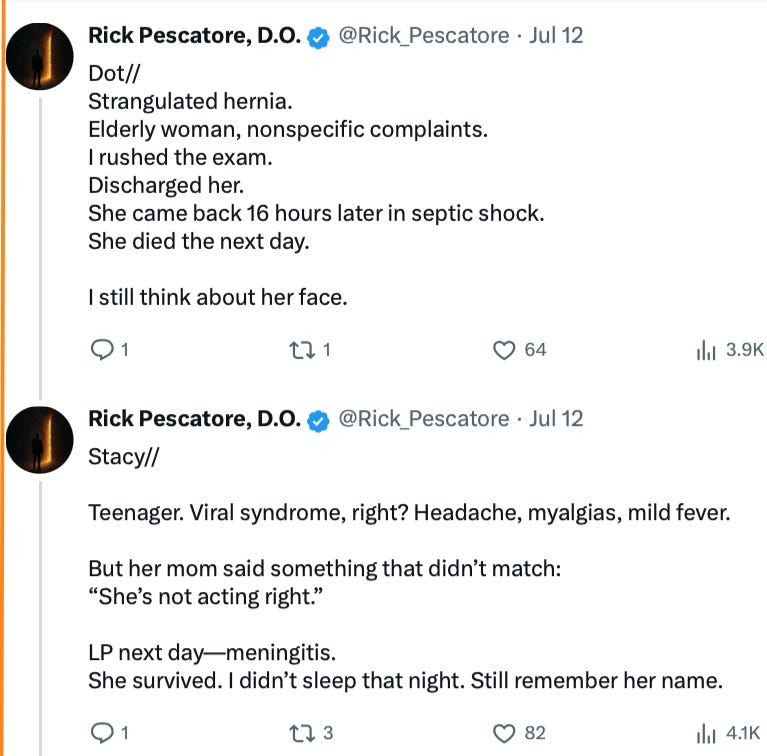
Former ER doc Rick Pescatore, D.O., tweets about some of the diagnoses he missed:
Though the pace and purpose of the ER can make even doctors of Pecatore’s caliber prone to tragic missed calls, diagnostic errors are rampant throughout medicine.
Santa, The Tooth Fairy, and Diagnostic Competence
In GOING MENOPOSTAL, I lay out three big myths we believe about our medical care—to the detriment of our health (and sometimes, our continuing “aliveness”).
Today’s catch? Diagnosis.
Myth #2: Doctors are highly trained in and skilled at diagnosis, the reasoning process to drill down to the underlying cause of a patient’s symptoms.
Reality: Dr. House ain’t home.
Diagnostic Error is Baked Into Medicine—from Med School On
Most med schools don’t teach even a single course on diagnosis “or how to avoid diagnostic error,” reports SUNY Stony Brook professor emeritus of medicine, Mark L. Graber, MD, in 2016.
We patients pay the price.
“The best estimate from autopsy studies is that there are 40,000 to 80,000 deaths a year from diagnostic error,” notes Graber (though he suspects vastly more patients are injured).
He explains that many of these errors involve doctors impulsively settling on a diagnosis because the symptoms “in front of them” happen to fit with a particular condition.
“Go no further medicine,” I call it.
A 2022 US Agency for Healthcare Research and Quality research review offers a per-ER estimate of diagnostic errors—and the resulting harm:
1 in 18 ED patients receiving an incorrect diagnosis, 1 in 50 suffering an adverse event, and 1 in 350 suffering permanent disability or death.
Heart attacks are among the most missed diagnoses.
And they are especially likely to be missed in women.
Meet Joe Plaque
Quick! Picture somebody having a heart attack.
Lemme guess: You rolled mental videotape of the “Hollywood heart attack”—some all-red-in-the-face businessman clutching his left arm and dropping like a sack of rocks.
On TV, heart attacks almost always strike men.
But over here in real life, heart attacks are the leading cause of death in women (and especially menopausal women), currently killing 1 in 5 and soon to take out 1 in 3. Strokes are not far behind, ranking as a leading cause of long-term disability in women and one of the top five causes of death.
Jenny From The Blockage
In both men and women, a heart attack starts with a blockage of blood flow to the heart, cutting off the oxygen transported in it that the heart needs to keep beating.
Kind of a big deal. A big GET THEE TO THE FUCKING EMERGENCY ROOM ASAP! deal.
Problematically, the cardiovascular disaster signs in women not only lack the dramatic intensity of the male clutch-’n’-drop, but they’re practically BEIGE.
Take the most common symptom in both men and women—chest pain. For men, the pain can be crushing—two tons of heart attack fun, like the house from the Wizard of Oz landed on a guy’s chest.
Women’s chest pain may be milder—and frankly, vague: a pressurized ache or squeezing or fullness in the chest that lasts a few minutes and then comes back.
With Hollywood Heart Attack as a cultural template, women shrug off symptoms like these as “just indigestion,” acid reflux, or stress—nothing to go to the ER over, reports nurse/scientist Cynthia Arslanian-Engoren, Ph.D.
Mama’s Mild-Mannered Myocardial Infarction
Say a woman does make her way to the ER. She’s likely to get vastly less aggressive (or even attentive) care than men—or get dismissed entirely: sent home with an Advil or a Benadryl or a scolding about wise and unwise places to order the clams.
(And no, sexism is not to blame!)
It seems many medical personnel also have the Hollywood heart attack in mind and are unaware of the comparatively bland way heart attack warning signs present in women.
Pain or discomfort in one or both arms and/or the jaw, neck, stomach, or back
Breaking out in a cold sweat
Nausea and vomiting
Shortness of breath
Dizziness or lightheadedness—feeling on the verge of passing out
Sudden extreme fatigue
Indigestion
Palpitations (fluttering feelings in the chest)
Anxiety (unrelated to anything specific)
Disturbed sleep: sudden difficulty falling asleep or staying asleep
Granted, these symptoms do show up in lots of “not a heart attack” situations.
But being clued in that they can point to “heart go boom” in a woman is vital, allowing us to err on the side of “Get thee to the ER!”—instead of defaulting to “it’s probably nothing” and delaying to the point there’s permanent heart damage.
We’re prone to do the latter. We humans are adorably pathetic, desperate to avoid the embarrassment we feel at being wrong—and especially theatrically wrong: wrong with screaming sirens, fire trucks, an ambulance, and a cast of firemen, paramedics, doctors, nurses, and a guy actually dying in the next bed.
Distrust—And Verify: In the ER and beyond
Avoiding the harms of diagnostic error takes a form of assertiveness I call “Defensive Patient-ing”—asking questions to suss out whether their diagnosis seems well-supported or whether their mental investigation ran the gamut from A to, uh, A.
Nine Questions
What is your specific diagnosis?
Could you walk me through your reasoning behind your diagnosis and the treatment you’re recommending?
Are there other conditions my symptoms might point to?
Are there tests would confirm or challenge this diagnosis?
Have you looked my lab numbers and health conditions and factored those into your diagnosis and treatment recommendation?
Please tell me all the risks, including less common risks, from the treatment or course of action you’re recommending.
Are there safer or less invasive treatments?
Do I need to do this now or could I wait or go without treatment?
Am I in any danger going home, and are there red flags that suggest I should come back fast?
Diagnostic Reasoning or Diagnostic Lazy Guess?
If a doctor can’t or won’t answer these questions—clearly and understandably—it’s a sign, and no, not that you’re stupid.
Consider that my psychiatrist explains complex neurology understandably to 5-year-olds—which takes being a doctor who truly understands complex neurology.
So, push for answers—satisfactory answers—until you get them. Which may take going to another doctor. Ask for a second opinion (your right by law and not the slightest bit rude to do).
Need time to think or call somebody you trust? Tell ‘em and take it—and refuse to be emotionally bullied into rushing.
They won’t like it. But they’ll respect you and wait for your answer.
That Voice in Your Head Deserves Your Attention
You know when something’s just not right with you—like that girl’s mother knew in Pescatore’s tweet above.
Insist on talking to other doctors or a supervisor (or a supervisor’s supervisor) until somebody agrees to check out your heart (or whatever).
While you’re doing it, give yourself props for being brave and maybe even refusing to be sent home to die.
That last bit might sound a little drama llama.
You’ll see from the story of a dear friend of mine that it’s anything but.
Wild Guess-Based Medicine

My friend and colleague, forensic psychologist Dr. Helen Smith, was 37 and in great shape—running regularly since the age of 12, working as a weight trainer at the NYU gym, and doing karate.
Suddenly, she couldn’t breathe.
“It was an awful feeling--I felt like I was smothering to death and going to pass out.”
Her husband called 911, and they told him to get her the nearest hospital.
“Despite the fact that I was short of breath and shaking like a leaf, the doctor decided I was allergic to something in the gym and gave me a shot of benadryl.”
On vacation a few weeks later, she got short of breath and could not walk. And she again went to the emergency room.
“Amazingly, while in the emergency room, a man in his thirties or forties came in with shortness of breath. He was whisked off for heart tests and his wife and two little children were there crying. I felt so sorry for them.”
She finally got doctors to do an EKG. The results suggested she’d had a heart attack—an MI, myocardial infarction, caused by a blockage of blood flow to part of the myocardium, one of the chambers of the heart.
At last! Time to save Helen’s life!
“A cardiologist came into the room, looked at the reading and shrugged, stating that many thin women in their 30's who were athletic had a similar reading. I took his word for it and left.”
She finally persuaded her regular doctor to look at her heart. He sent her for tests—and called her and told her to get to the hospital PRONTO.
She was with her dad, who raced her to the hospital.
When they got there, the orderlies told him to get in the wheelchair—figuring that he was the one with the heart about to blow.
“I would have laughed myself silly if I had not been so ill. I had tests including a heart cath that helps doctors to see inside the heart.
Later, when I was back in my room, the cardiologist came in and told me that I had suffered from a heart attack and also had a ventricular aneurysm (a ballooned out area of the heart) as a result of not resting my heart after the heart attack.
I had been told that I had panic disorder so I thought that exercise would be good.”
Eventually, they diagnosed her with what’s basically an electrical malfunction in the heart, ventricular tachycardia: an irregular heart rhythm in which the lower chamber of the heart beats dangerously fast—too fast to pump well, starving the body of oxygen (that travels in blood).
Electrical problems get electrical solutions: an implanted ICD, a defibrillator that will shock her heart back into a healthy rhythm if it goes off the rails.
I also received the life-saving drug Tikosyn, which is so potent, I had to take it for five days in the hospital to make sure I could tolerate it.
For the first time in years, I feel almost normal. I give thanks everyday for the amazing advances in heart research over the past 15 years. I know it sounds cliche, but I feel lucky just to be alive. When other people in their thirties and forties complain about their aches and pains, I just laugh--I feel lucky to get up in the morning without feeling dizzy or nearly fainting.

The Mundane Objects Of My Ongoing Tragedy
(11:50 am, Nov 7, 2025, Kaiser Permanente West Los Angeles Medical Center.)

I may never walk normally again.
That’s a tin of herring I can no longer open.
My horrifically negligent cornea surgeon did this to me. The worst thing anyone has ever done to me.
Upon completing my first corneal endothelium transplant March 10, 2025, she prescribed me a corticosteroid eye drop, prednisolone acetate, and what amounted to systemic levels of a fluoroquinolone antibiotic. (Ofloxacin and then Moxifloxacin.)
Unbeknownst to me, this drug risks tendon damage, including tendon rupture from “routine movement,” and nerve damage that takes your ability to balance and walk from you. (FDA Black Box 2008 and 2016, respectively.) And don’t forget that groovy aortic dissection!
Zero informed consent. Zero disclosure of risks. Making this prescription medical battery.
On the morning of October 4, the symptoms hit: Two terribly painful episodes of trigger finger, a disorder I did not have. The symptoms have gotten progressively worse—throughout my body. My fingers are so stiff and painful that I often can’t even type till 8:30 or 9 p.m.
On October 7, at 1:45 a.m., I notified Kaiser (via a PDF to my cornea surgeon, sent through KP’s portal) that I required referral to an “appropriate expert specialist” with fluoroquinolone expertise and diagnostic MRIs to investigate the state of my tendons so I could avoid or minimize movement of those that were damaged, torn, or at risk.
I have spent since October 4 day and night fighting Kaiser Permanente for the vital diagnostic imaging and nerve tests I need to possibly mitigate further harm. It is November 14, Friday, 2:05 a.m., as I write this.
Kaiser has violated “timely access” rules of the California Department of Managed Healthcare through much of October by not expediting the diagnostic appointment in a situation with urgent catastrophic risk. $2500 fine a day at the 96 hour point from 1:45 a.m. October 7.
I now have a torn shoulder tendon, torn biceps tendon, a torn ankle tendon, a partially detached (from the bone) ankle tendon, and the edema (swelling) around the Achilles tendons that precedes rupture. My friend Heather Heying will tell you how much fun that is. As is having prostate cancer like Scott Adams and having simply evil denials of care by Kaiser.
The Doctor Ate My Homework
I don’t miss deadlines.
But I thought about all of you who subscribed—many of you I know as my beloved column readers, blog commenters, Going Menopostal readers, and more.
I thought about Raddy from blogland, and though he’d tell me to take care of my health first. And I think that’s what a lot of you would say.
It’s been horrific. And I’ll tell the story better soon. And it’s unbelievable. And I’m really proud of myself for the ways I’ve fought to get the care Kaiser is denying me.
Fiercely, daily, “Amy Alkoning things into happening.”
And there have been some major heroes in this, including my gynecologist (the single biggest hero), gyno boss in the book, the entire West LA department of radiology, Sean who runs the lab, the neuro nurses, a janitor with a missing front tooth.
I have fought in incredible ways that no patient could, as both a medical expert and expert in delivery of care, the laws and codes surrounding that, and more. When I’ve had more sleep and gotten the last few tests I’m fighting for, I will be posting shorter posts and more frequently.
Also, I will use this to help other FW-injured patients. And I already am. As I’ve going through these battles, I regularly feel sick about other patients—who have zero capacity to muster the scientific gotchas I use. And then, a major breakthrough.
On Thursday, I figured out the nut of this—an incredible nut—that should eliminate the need for patients to do more than wave a page of words I give them at their providers. (Pro tip to KP: Don’t fuck with a woman who wakes up to FQ injury with thoughts of Knox v. Keene and other delivery of care cases flying around in her head like irate Sugar Plum Fairies!)
This has also led to a whole slew of ideas on how we can all proactively avoid medical harm, and these require no medical knowledge and are pretty exciting.
To see more on this, Twitter searches: amyalkon fluoroquinolone, amyalkon blackbox, amyalkon black box.
Warning: These are not necessarily all that coherent because this fight is so massive and hard every hour of every day, and keep staying up til 3, 4, 5 a.m. to file correctly with the Department of Managed Healthcare and write rebuttals to Kaiser.
Oh, and did I mention writing my own MRIs that my fucking hero of a gynecologist has been putting in for me? At the behest of truly wonderful gyno boss, who said he could help me.
Unfortunately, he can only order below the ovaries! So I am left to this day to fight Kaiser for the beyond urgent hand and wrist MRI—correctly written (by me)—and the urgent 3mm skin punch biopsies for small fiber neuropathy.
They keep denying these (and more) and delaying or just doing nothing about other necessary elements of diagnosis and care.
They think this is a big win for them, having not a bent clue about how wildly stupid it is to keep me hanging around when you’re hiding medical evil to sick and suffering people behind a bureaucratic veneer.
Help Me Help You! (Please Donate.)

I need your financial support for SCIENCE MADE PRACTICAL to continue my 30-year mission of putting out rigorous, highly practical applied science.
You’ll be helping fund my deep dives into research across disciplines and the doable applied science solutions I come up with for my readers.
Ways to Donate:
• PayPal (one-time—or monthly or yearly donation)
• Credit or debit card (one-time donation)
• To use another method, please email: info@amyalkon.net

Buy GOING MENOPOSTAL:
What you (and your doctor) need to know about the real science of menopause and perimenopause
“This is a rigorous and meticulous guide to everything related to menopause. … Alkon does a tremendous job of breaking down scientific facts for everyday readers. … Her smart, thoughtful accounts of her own experiences lend a feeling of camaraderie to the book.” —Kirkus Reviews
I'm so sorry to read about what you're going through.
One piece of advice from me to everyone who has the option: DO NOT sign up for an HMO a.k.a. "managed care" plan. Get a PPO plan instead. You will pay a bit more, but the flexibility and freedom to choose your own physicians is worth it.